Sepsis and Food Poisoning: Treatment and Compensation
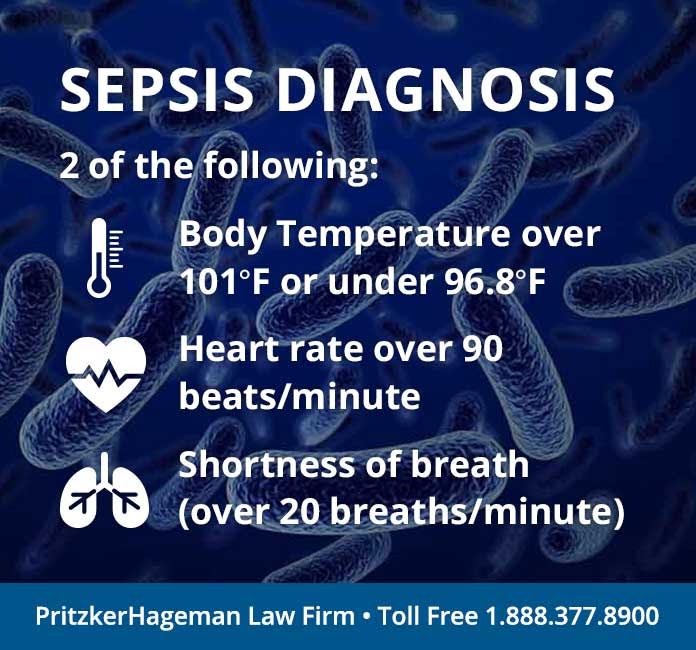
Most people do not know that food poisoning is an infection. What happens is a dangerous pathogen (Campylobacter, E. coli, Salmonella, Vibrio) gets into food. When that food is eaten, the pathogen can cause an infection that manifests as diarrhea, vomiting, abdominal cramping and sometimes fever. If this infection is transported in the blood to other areas of the body (kidneys, brain, heart, pancreas, etc.) the infection is then septic (body-wide), and the patient has sepsis. If the sepsis causes an extreme drop in blood pressure, the result is septic shock and possible death.
Attorney Fred Pritzker
“Our lawyers have represented many outbreak victims who developed sepsis,” said Fred Pritzker, a national attorney who has won millions for food poisoning victims. “In some of the cases, our client did not survive, and it went from a personal injury case to a wrongful death case.”
“If the sepsis moves into septic shock, at least one organ generally fails. With food poisoning, the kidneys are the most at risk for failure.”
Our attorneys recently recovered $4.5 million for a young woman who ate steak contaminated with E. coli bacteria, developed hemolytic uremic syndrome (HUS), suffered kidney failure and is permanently injured. They sued the restaurant where their client had eaten the steak. You can contact Fred about your food poisoning claim at 1-888-377-8900 (toll-free).
New Study Looks at Sepsis Treatment
A new study funded by the National Institute of General Medical Sciences (NIGMS), a component of the National Institutes of Health (NIH), found that the survival rate of patients with septic shock was the same regardless of whether they received the usual high-level standard of care or less expensive care. The study was conducted over a period of 5 years at 31 hospital emergency departments throughout the United States.
“Sepsis affects more than 800,000 Americans annually and is the ninth leading cause of disease-related deaths,” according to the Centers for Disease Control and Prevention (CDC).
The study looked at 3 approaches to sepsis treatment:
Early Goal-Directed Therapy: Doctors inserted a central venous catheter—a long, thin tube placed close to a patient’s heart—to continuously monitor blood pressure and blood oxygen levels. For the first six hours of care, doctors kept these levels within tightly specified ranges using intravenous fluids, cardiovascular drugs and blood transfusions.
Protocolized Standard Care: This less invasive treatment did not require central venous catheter insertion. Doctors used standard bedside measures like blood pressure (taken using an arm cuff), heart rate and clinical judgment to evaluate patient status and guide treatment decisions. Doctors kept patient blood pressure and fluid levels within specified ranges for the first six hours of care.
Standard Care: Patients received the standard high level of care typically given at an emergency department at an academic hospital.
The study researchers found that the 3 approaches to treatment produced similar results for some patient outcomes, including the following: survival at 60 days, 90 days and one year; heart and lung function; length of hospital stay; and a standardized measurement of health status at discharge.
The study researchers concluded that the key to recovery is prompt diagnosis and adequate treatment with fluid and antibiotics, not necessarily more invasive care. With some foodborne pathogens, like E. coli, this poses a problem, because use of antibiotics can cause the patient to develop HUS. In addition, some foodborne pathogens are now antibiotic-resistant.
We would like to see a similar study done strictly with food poisoning victims who have developed sepsis before any treatment changes are made.
The results of the study discussed above have been published in The New England Journal of Medicine: March 18, 2014DOI: 10.1056/NEJMoa1401602